Malignant Otitis Externa (Skull Base Osteomyelitis)
💎 Buy my Premium ENT Notes
Instant access to 200+ high-yield ENT notes. Your purchase includes all future updates.
🇮🇳 For Indian Students
· To buy all my notes, click here💡 This post is a free outline of my YouTube video. Get my full handwritten notes using the links above.
🧠 Malignant Otitis Externa (Skull Base Osteomyelitis)
🌬 What is Malignant Otitis Externa?
Malignant Otitis Externa is an invasive bacterial infection that starts in the External Auditory Canal (EAC) and spreads to involve the skull base and surrounding soft tissues.
It is typically seen in long-standing diabetic or immunocompromised patients.
✨ Why is Malignant Otitis Externa called "Malignant"?
🦠 Pathology of Malignant Otitis Externa
-
Mode of Entry: Usually starts with self-inflicted trauma to the EAC, followed by a Pseudomonas infection.
-
Spread: This is the end stage of severe EAC infection. Infection spreads quickly via congenital defects in the EAC floor (e.g., fissures of Santorini) and the haversian system of compact bone.
🔬 What is the pathogenesis of Malignant Otitis Externa?
🔬 Why is Pseudomonas highly invasive in Malignant Otitis Externa? What are it's mode of action?
🌍 Epidemiology and Predisposing Factors of Malignant Otitis Externa
-
Age: Most common in old age.
-
Underlying Conditions (Crucial Predisposing Factors):
-
Uncontrolled Diabetes Mellitus
-
Other Immunocompromised states: Immunodeficiencies, AIDS, Chemotherapy, etc.
-
Malignancy of the temporal bone.
-
Histiocytosis.
-
What is the most common predisposing factor of Malignant Otitis Externa? Why?
🦠 Causative Organisms of Malignant Otitis Externa
-
Most common: Pseudomonas aeruginosa (accounts for the vast majority of cases).
-
Other bacteria: Staphylococcus aureus.
-
Fungi: Aspergillus, Candida (rare fungal causes).
📋 Clinical Features of Malignant Otitis Externa
-
Previous History: Often a history of recurrent or poorly controlled Otitis Externa.
-
Ear Pain (Otalgia) - Hallmark Symptom
What are the typical characteristics of Ear pain in Malignant Otitis Externa?
-
Ear Discharge (Otorrhea)
-
Granulation Tissue - Hallmark Sign
Where is granulation tissue seen on clinical examination in Malignant Otitis Externa?
-
Necrotic Pockets: May be seen around the granulation tissue.
-
EAC: Edematous, narrowed, potentially obliterated. Sagging of canal wall may occur.
-
Spread to Soft Tissues: Swelling and tenderness in the surrounding areas (e.g., pre-auricular, post-auricular, parotid region, cervical region).
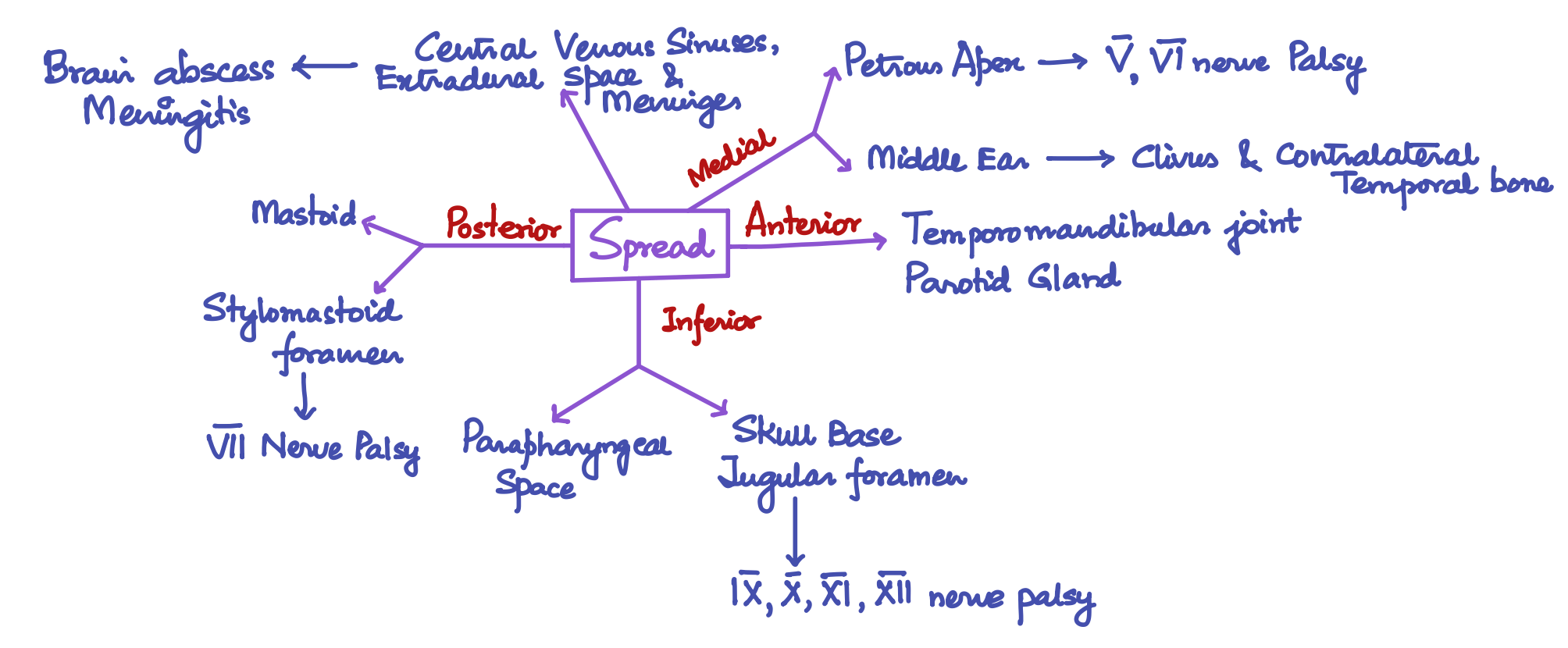
Cranial Nerve Involvement:
Spread of infection along the skull base can directly involve cranial nerves:
- CN V (Trigeminal) & CN VI (Abducens)
- CN VII (Facial)
- CN IX (Glossopharyngeal), CN X (Vagus), CN XI (Accessory), CN XII (Hypoglossal)
Which Cranial nerve involvement has the best prognosis?
📊 Staging of Malignant Otitis Externa
A common staging system (Chandler's) helps classify disease severity:
-
Stage 1: Clinical evidence of disease with soft tissue infection beyond the EAC. Negative Technetium-99 bone scan.
-
Stage 2: Soft tissue infection beyond the EAC. Positive Technetium-99 bone scan.
-
Stage 3: Soft tissue infection beyond the EAC + Positive Technetium-99 bone scan + Cranial nerve paralysis.
- Stage 3a: Single cranial nerve involved.
- Stage 3b: Multiple cranial nerves involved.
-
Stage 4: Disease involves the soft tissue, bone, and leads to intracranial complications (meningitis, empyema, sinus thrombosis, brain abscess).
Spread of Malignant Otitis Externa
🩺 Diagnosis of Malignant Otitis Externa
The diagnosis is primarily clinical, strongly suspected based on the characteristic triad:
- Elderly diabetic or immunocompromised patient
- Severe, often nocturnal, deep-seated otalgia
- Granulation tissue in the EAC at the bony-cartilaginous junction
🔬 Investigations of Malignant Otitis Externa
-
Blood Tests: Elevated ESR and CRP
-
Biopsy: Biopsy of the granulation tissue in the EAC is essential to rule out malignancy (EAC carcinoma) and confirm the inflammatory/infective nature.
-
Imaging:
- CT Scan
- MRI
- MR Venography
- MR Angiography
What are the Indications of performing CT scan, MRI scan, MR Venography and MR Angiography?
- Nuclear Scans:
Technetium-99 (Tc-99) Bone Scan: Taken up by osteoclasts/blasts. Becomes positive within 1-2 days of osteomyelitis onset.
What is the importance of Technetium-99 (Tc-99) Bone Scan?
Gallium-67 (Ga-67) Scan: Taken up by monocytes/reticuloendothelial cells. Indicates soft tissue infection and active inflammation (shows "hot spots" in infected areas).
What is the purpose of Gallium-67 (Ga-67) Scan?
Indium-111 (In-111) Leukocyte Scan: More specific for active infection/inflammation (shows where WBCs are concentrating). Can supplement Gallium scan.
🏥 Treatment of Malignant Otitis Externa
-
Control Predisposing Condition: Strict control of Diabetes Mellitus is paramount. Address other immunocompromised states or underlying malignancies.
-
Local Treatment / Oral Toileting: Daily meticulous cleaning and debridement of the EAC to remove purulent discharge, granulation tissue, debris, and bone fragments.
-
Antibiotics: The mainstay of treatment. Usually given intravenously for 6-8 weeks, sometimes followed by oral antibiotics for several months.
- Initially, broad-spectrum coverage targeting Pseudomonas is essential.
- Often combination therapy.
What are the first line and second line antibiotics used in treating Malignant Otitis Externa?
What is the Antifungal drug used if a fungal etiology is suspected in Mallignant Otitis Externa?
-
Analgesics: Essential for severe pain control (e.g., Acetaminophen, often stronger required initially).
-
Hyperbaric Oxygen Therapy (HBOT): Can be a valuable adjunct, especially in refractory cases or those with poor vascularity (like diabetics).
What is the mechanism of action of Hyperbaric Oxygen Therapy in Malignant Otitis externa?
What are the treatment settings of Hyperbaric Oxygen Therapy in Malignant Otitis externa?
-
Surgery: Generally avoided or minimized if possible.
- Limited debridement of necrotic bone and granulation tissue.
- Drainage of abscesses (if formed).
- More extensive surgery is only performed if infection progresses despite maximal medical therapy.
Why is surgery avoided in Malignant Otitis Externa?
📈 Monitoring Response to Treatment:
What is the Earliest Clinical Sign of Response?
What is the Earliest Investigation Response?
Which scan is used to monitor treatment response in patients of Malignant Otitis Externa? Why?
🤕 Prognosis of Malignant Otitis Externa
-
Prognosis: Can be poor, especially in advanced stages or with significant comorbidities. Mortality rates can be high without aggressive treatment. Recurrence is common, often due to inadequate initial therapy.
-
Recurrence: May present as recurrent headaches and otalgia, not necessarily otorrhea.
⚠️ Complications of Malignant Otitis Externa
- External nose deformity
- Vestibular stenosis
- Cranial Nerve Palsies: CN VII, V, VI, IX, X, XI, XII
- Sigmoid sinus thrombosis
- Internal carotid artery thrombosis
- Intracranial Complications: Meningitis, Brain Abscess, Empyema
🤔 Differential Diagnosis of Malignant Otitis Externa
Consider other conditions that can cause EAC lesions, skull base involvement, or facial/ear pain:
- External Auditory Canal Malignancy.
- Granulomatous diseases (e.g., Sarcoidosis, Wegener's Granulomatosis).
- Paget's Disease.
- Nasopharyngeal Malignancy.
- Clival lesions.
- Fibrous Dysplasia.
- Simple Otitis Externa
- Referred Otalgia
📝 All topics and questions from this post are explained in detail in my Premium ENT Notes, which are designed for clinical understanding and exam success.
Residency is hard enough. Studying for it shouldn't be 😊
💎 Buy my Premium ENT Notes
Instant access to 200+ high-yield ENT notes. Your purchase includes all future updates.
🇮🇳 For Indian Students
· To buy all my notes, click here